Update on ATA’s Policy & Advocacy Work
Telehealth’s value is being realized thanks to the cohesive voice of the industry through the ATA and our members and partners
As we approach the half year mark for state legislatures, and four months with a new Administration and new Congress, one thing is clear: Telehealth’s value is being realized thanks to the cohesive voice of the industry through the ATA and our members and partners. You know that temporary changes at the state and federal levels – when made permanent – would positively transform our nation’s health system. The purpose of this note is to provide a brief update on activity and on our work to date which I encourage you each to share with fellow executives in your organization.
The Biden Administration President Biden and his administration have been on record in support of telehealth during the campaign and since taking office. In fact, US Department of Health and Human Services (HHS) Secretary Xavier Becerra stated during his confirmation hearing: “…. If we don’t learn from COVID that telehealth can help save lives, then we’re going to be in trouble. So, I think we’re going to advance.” The public health emergency (PHE) is expected to be continued by the Biden administration for at least the duration of 2021. Importantly, while the administration has a number of tools at their disposal in support of telehealth, if we are going to ensure Americans continue to have access to telehealth after the pandemic ends, Congress must act.
Telehealth and the 117th Congress Legislation has been introduced by our congressional telehealth champions that seeks to ensure Medicare beneficiaries maintain access to telehealth after the PHE ends. Three comprehensive bills — the CONNECT for Health Act, the Telehealth Modernization Act, and the Protecting Access to Post-COVID-19 Telehealth Act — each have nuanced distinctions regarding policy provisions but demonstrate bipartisan support on Capitol Hill. However, we anticipate that passing standalone legislation may not be possible and our policies may be included in a broader package – i.e., an appropriations or extenders package, which could be several months away. The ATA is also working with Congressional offices on introduction of potential legislation that would repeal the in-person requirement that is now attached to telemental health. This provision, passed into law at the end of 2020, is clinically unnecessary, denies individuals access to needed care, and is not replicated in any state. Please see our federal telehealth legislative tracker.
![]()
Medicare Payment Advisory Commission (MedPAC) Chapter on Telehealth In their March 2021 report to Congress on Medicare payment policy, MedPAC recognized the importance of telehealth during the PHE and the need for policy changes to ensure access to telehealth post-pandemic. MedPAC referenced telehealth benefits and cited their annual beneficiary survey, reporting overwhelmingly high satisfaction rates for telehealth. While MedPAC did not recommend permanently maintaining telehealth flexibilities, it did propose that Congress extend flexibilities for one to two years after the PHE to “gather more evidence about the impact of telehealth on access, quality, and cost.” This year, there is a real possibility Congress may end up extending flexibilities past the end of the PHE rather than making the flexibilities permanent.
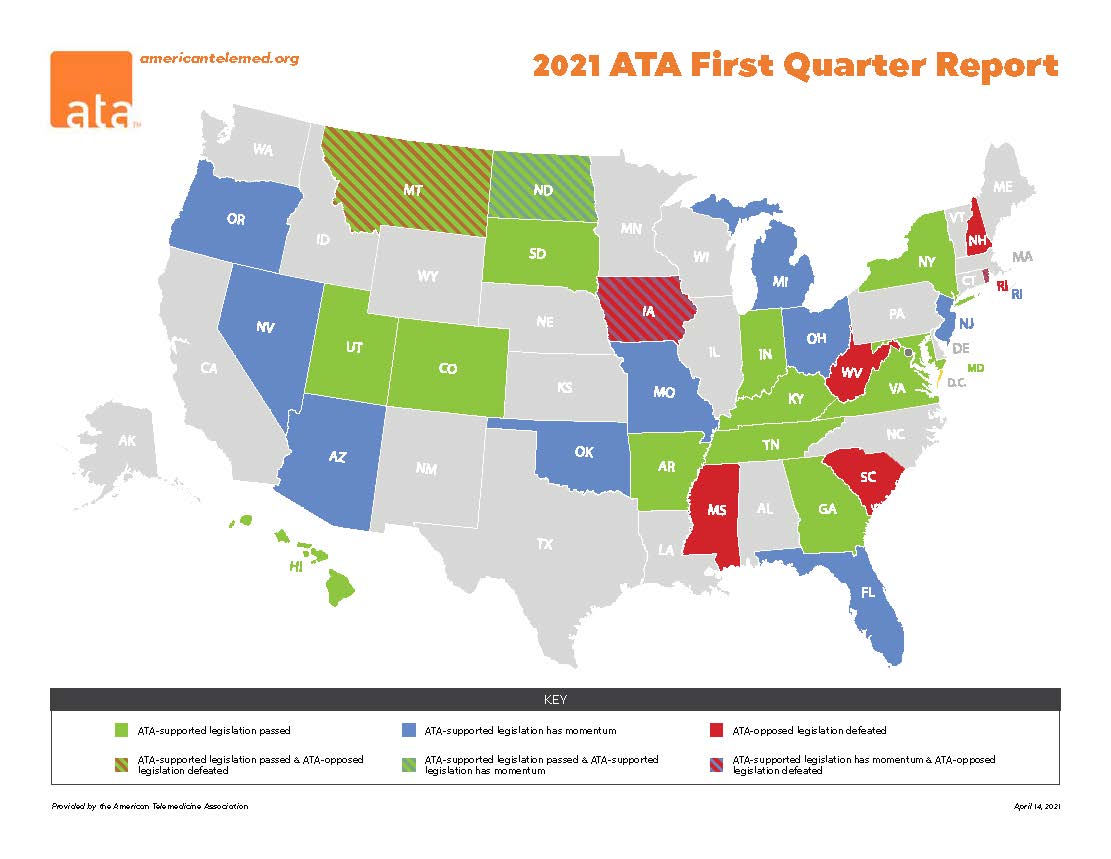
State level activity We track critical state legislation, as over 600 bills were filed related to telehealth in all 50 states. The ATA has commented on over 60 bills since the beginning of 2021 and scored an important win in Arkansas last month. Our team has also delivered testimony in key states and for the Uniform Law Commission’s Committee on Telehealth. For a comprehensive overview of state legislation, please see our state legislative tracker and map.
The trends we’ve seen in state legislation include:
- New and/or revised telehealth practice standards (definitions, permissible technologies, recordkeeping, providers eligible to use it)
- Licensure portability and flexibilities (including compacts and reciprocity akin to what existed under waiver authorities)
- Private payor coverage and reimbursement (i.e. parity, including for audio-only)
- Public payor coverage (comparable to federal, questions about eligible providers, services, and patient locations)
- Broadband connectivity + grants or telehealth (addressing digital divide issues)
We believe the momentum seen in state capitals can be parlayed into success at the federal level by communicating to federal policymakers the following:
- By passing permanent policies into law, state legislatures and governors are ensuring telehealth flexibilities do not go away post-pandemic – this is particularly relevant for Congressional offices representing states that have acted
- There are layers of protection and accountability for patients in place already through state licensure boards and state regulatory agencies – federal policymakers do not need to recreate the wheel through federal action/guardrails
- No state law replicates the telemental health in-person requirement, understanding that such policies deny their citizens access to healthcare
I hope you find this update helpful which you can also download in .pdf format. We could not be as influential as we are on behalf of the industry without your continued support and extend our special thanks to our Next Steps into 2021 Campaign partners. Please contact me or Kyle Zebley, who leads our policy work, should you have questions. You can reach us at ann@americantelemed.org and kzebley@americantelemed.org.
Ann Mond Johnson is the chief executive officer of the American Telemedicine Association (ATA), working to transform health and care through enhanced, efficient delivery via telehealth.
View this post on https://f.hubspotusercontent30.net/hubfs/5096139/Files/Campaign/Update%20on%20the%20ATAs%20Policy%20Work%20Memo_5.19.2021.pdf
